Completing the Picture: Clavicle Landmarking, Curvature, and Safety for Shoulder Injections (Part 2)
I’m Dr. David Wang of RPI, continuing our focused discussion on accurate palpation-based marking for shoulder injections. This installment zooms in on the clavicle’s curvature, the posterior border, and the V landmark—crucial for accurate, safe injections near the clavicle and superior shoulder region.
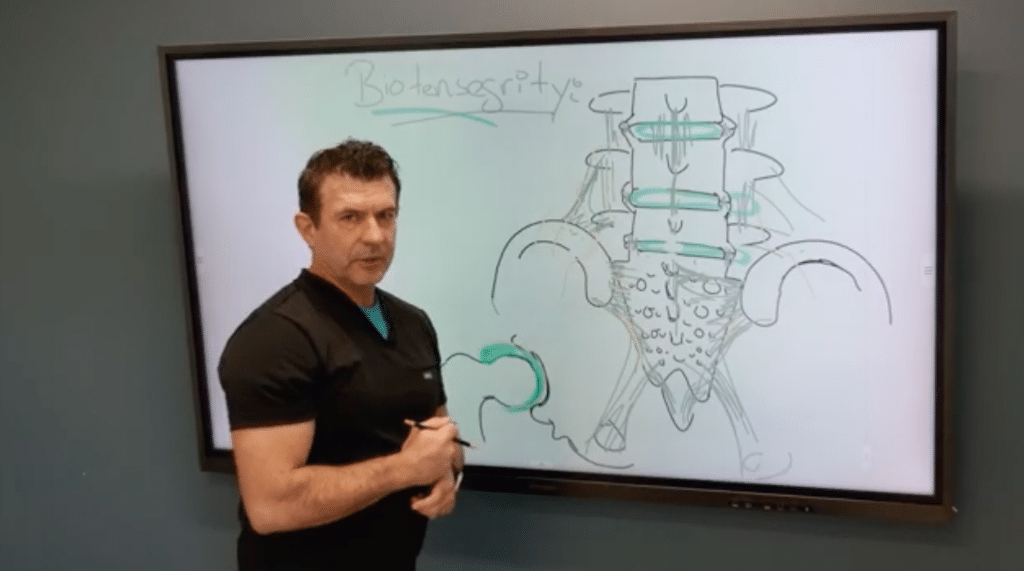
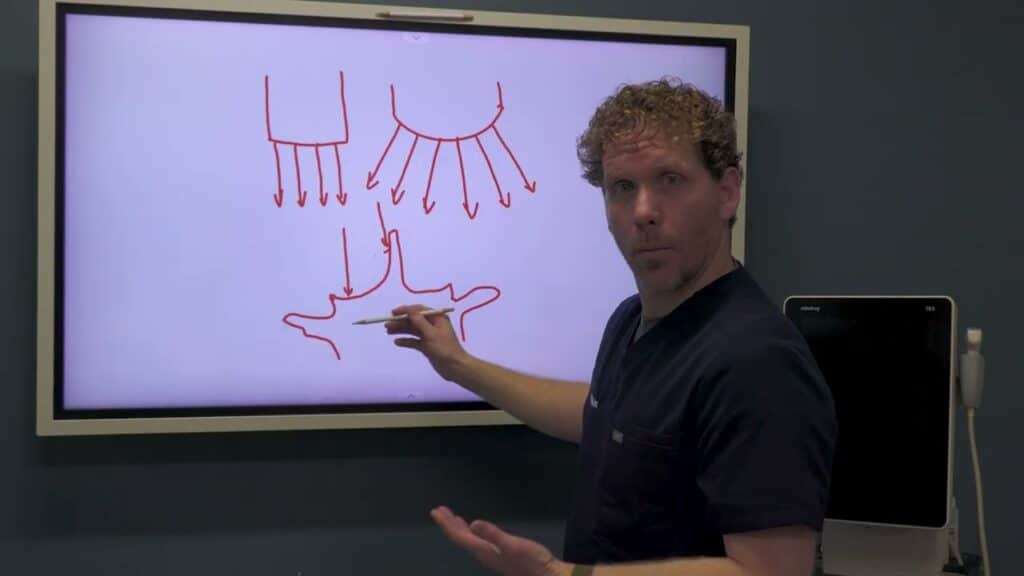
The clavicle is not a uniform cylinder. The medial aspect remains relatively rounded, while the lateral portion flattens and widens, creating a dynamic landmark landscape. The posterior border of the distal clavicle sits further back than learners expect, largely due to the overlying trapezius and the clavicle’s curved anatomy. When marking, it’s essential to preserve the clavicle’s natural S-curve and to identify the V-shaped posterolateral clavicle corner, which marks the entry point for superior injections toward the labrum.
A critical error to avoid is misidentifying the coracoid process as part of the clavicle. The coracoid is a distinct structure, and misidentifying it can derail marking accuracy. By maintaining awareness of the clavicle’s curvature and its posterior border, you’ll be better equipped to target the superior shoulder region safely and effectively. To implement this in practice, mark the medial clavicle edge that truly reflects the medial boundary, outline the S-curve and posterior border, and identify the V landmark that guides injections toward the labrum region. When used with ultrasound guidance, this approach improves accuracy and reduces tissue misplacement.