A Practical Approach to the Low Back: Targeting Fascia, Ligaments, and Tendinous Attachments (Part 3)
For clinicians who treat low back pain, a paradigm shift is underway: we can move beyond primarily targeting discs and nerves and toward understanding the fascia, ligaments, and muscle-tendon attachments that fundamentally stabilize the lumbar region. When we focus on these structures—the thoracolumbar fascia, attachments at the iliac crest, and the fascial connections surrounding the lumbar spine—we open up a broader, more effective set of diagnostic and therapeutic options. This approach helps explain why some patients who have failed epidurals or traditional corticosteroid therapies still improve with regenerative or targeted soft-tissue treatments. It also provides a framework for explaining to patients why pain may persist even when imaging looks relatively benign.
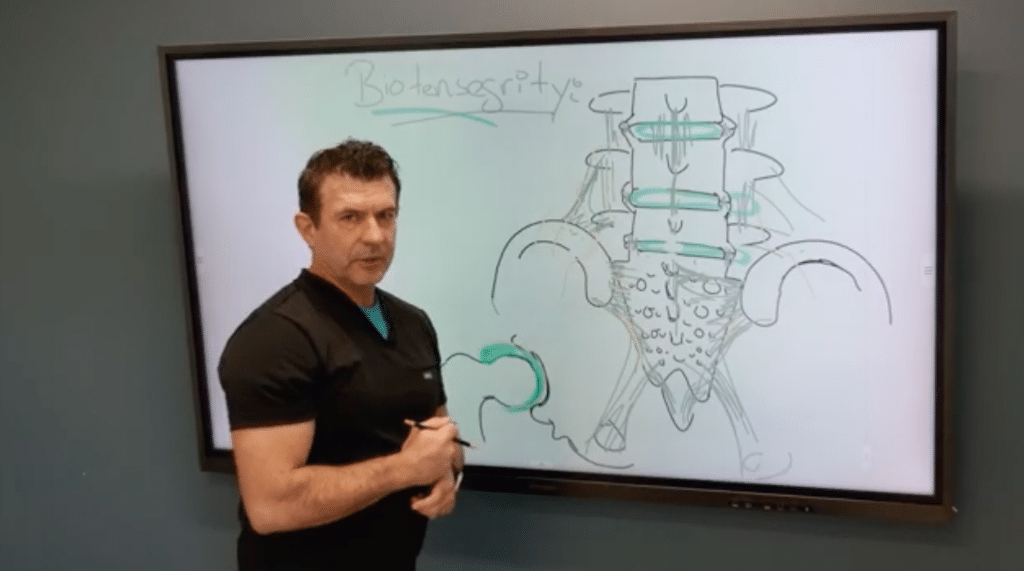
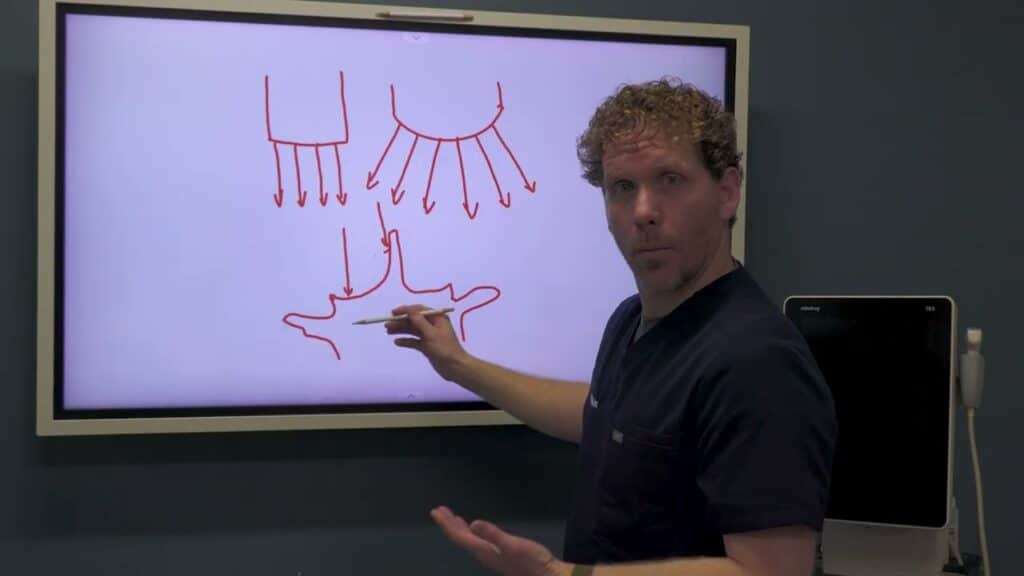
Begin with fascia as a central concept. The thoracolumbar fascia is more than a passive cover; it forms a critical plane that transmits forces between the abdominal wall, the back muscles, and the spine. Chronic tension in this fascia can create tugging forces at bony landmarks such as the iliac crest and the posterior lumbar region. Over time, sustained tension can lead to calcifications, microtears, or degenerative changes at attachments. When evaluating a patient, ask: Is there a pattern of midline or crest-located pain that worsens with movement or fascia-tension activities? Do imaging studies show calcifications or cystic changes near the crest or along the fascia’s paths? These clues guide you toward a management plan that includes addressing fascial integrity, not just nerve or disc pathology.
Understanding attachments matters because they are the sites where muscles and ligaments anchor to bone. The spine is a dynamic system: muscles attach to vertebrae, ligaments anchor to bone surfaces, and fascia blends between anterior and posterior structures. In the low back, these attachments can become symptomatic when tense, torn, or calcified. For example, the area around the iliac crest and lateral trochanter can show feathery calcifications on radiographs, which reflect long-standing attachment stress. These findings are not incidental; they point to mechanical drivers of pain that may respond to targeted regenerative or rehabilitative strategies. Ultrasound and advanced imaging help visualize these attachments and the fascia’s boundaries. By mapping these landmarks—iliac crests, spinous processes, transverse processes, and the sacral edges—you can guide injections or tissue-modifying therapies to the precise sites contributing to pain.
Another key piece is recognizing that pain generators in the low back are often overlapping. A patient’s pain may emanate from a combination of disc, facet joints, nerve structures, and soft-tissue attachments. When a steroid epidural fails to produce lasting relief, it’s a signal to reassess: could fascia or tendon-to-bone attachments be driving the pain? In these scenarios, therapies that target soft tissue—platelet-rich plasma (PRP), platelet-poor plasma (PPP), or stem-cell–based strategies—offer the potential to regenerate or repair damaged fascia and tendon interfaces. Early-stage evidence and clinical experience support the safety and utility of these approaches for soft tissue and ligamentous pathology, provided they are applied with careful patient selection and ultrasound guidance.
Practical steps to implement in your practice begin with a thorough but focused history and a biomechanical exam. Ask patients about activities that tension the thoracolumbar fascia—lifting, twisting, or sudden hip-flexor-dominant movements. Observe movement patterns and palpate along the crest, the transverse and spinous processes, and the posterior lumbar muscles for tenderness or bony wear. Use ultrasound not only to visualize soft tissue integrity but also to identify the fascia’s planes and attachment points. When you suspect fascial or attachment-driven pain, consider regenerative injections to the relevant fascial interfaces and tendon attachments. Platelet-rich products can be introduced to support tissue healing, while ensuring that you document responses carefully to build a personalized, iterative treatment plan.
In addition to regenerative approaches, don’t underestimate the value of foundational modalities: physical therapy focused on stabilizing the posterior elements, gradual loading strategies that promote tissue remodeling, and targeted manual therapies to restore fascial glide and reduce trigger points. A multimodal plan often yields the best outcomes because it addresses both the mechanical basis of pain and the tissue-level healing processes. If imaging or diagnostic blocks reveal that pain is driven by deeper structures, convert insights into a staged plan that escalates from conservative care to targeted interventions as needed. The overarching goal remains consistent: reduce pain, improve function, and restore durable mechanical health to the lumbar region.
Education is a critical companion to treatment. Help patients understand that the low back is a complex, integrated system, where fascia, muscles, ligaments, and bones all contribute to stability and movement. Framing pain within this network helps patients participate in a long-term plan rather than seeking a quick fix. Share the rationale for regenerative therapies and how they complement exercise, posture retraining, and ergonomic modifications. With proper patient education, you can set realistic expectations and improve adherence to a comprehensive treatment program.
As you advance this approach, you’ll gain a more nuanced map of the low back’s soft tissue architecture. You’ll be better equipped to select injection targets with ultrasound guidance, plan a staged treatment sequence, and combine regenerative therapies with rehabilitation to maximize outcomes. Although every patient is unique, the underlying principle remains universal: by healing the tissue interfaces—the fascia, ligaments, and tendon attachments that anchor the lumbar spine—you address the root mechanical drivers of pain and pave the way for lasting improvement.