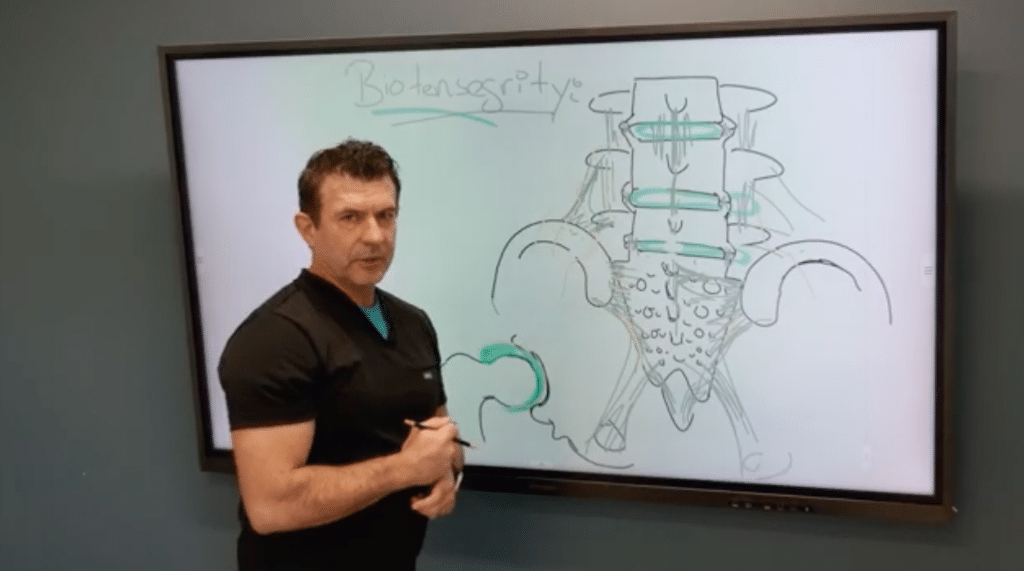
Thoracolumbar Fascia at the PSIS: Ultrasound Diagnosis and Injection Guide
Axial low back pain that patients localize with a fingertip over one or both posterior superior iliac spines (PSIS) often implicates the thoracolumbar fascia (TLF). With ultrasound, you can reliably identify the PSIS, visualize both deep and superficial TLF bands, and target regenerative injections to the most pathologic tissue.
Clinical pattern
When asked, many patients point to “that spot” just over the PSIS on one or both sides. This aligns with the primary TLF attachment on the posterior-superior aspect of the ilium. Reproducible point tenderness here—especially with resisted trunk motions or prolonged standing—raises suspicion for TLF strain/degeneration.
Find the PSIS fast
If surface anatomy is challenging (e.g., higher BMI), use the thenar eminence as a broad palpation tool to locate the bony prominence. Set your fingertips where the thenar eminence lands to fine-tune position.
Ultrasound roadmap
1) Orient in transverse (short axis) to confirm PSIS.
- On screen, set medial = right and lateral = left (match your machine conventions).
- Identify the superficial PSIS cortex.
2) Deep band (long axis over the PSIS ridge).
- Pivot to long axis so the PSIS cortex spans the screen.
- Scan medially↔laterally to survey the deep TLF attachment.
- Pathology clues: cortical irregularity, hypoechoic change at the enthesis, or loss of crisp fibrillar interfaces consistent with chronic strain/degeneration.
- Injection: in-plane or out-of-plane tracking along the ridge where the deep band anchors.
3) Superficial band (rotate 60–90°).
- Pivot the superficial end medially until a bright, thick, superficial band comes into view descending to the PSIS.
- Pathology is often more frequent here: look for hypoechoic banding, focal calcific/enthesophyte change, or disrupted echotexture.
- Sweep to capture the worst segment—many patients show maximal findings slightly lateral to midline.
Injection technique pearls
- Target the most abnormal segment (superficial more often symptomatic); treat the deep band when cortical irregularity/hypoechogenicity is prominent at the ridge.
- Keep the needle in-plane when feasible for precise deposition; use small test volumes to confirm plane/spread.
- Hydrodissect along the diseased layer to restore glide, then deliver your chosen regenerative solution (e.g., dextrose, PRP) into the fascial plane/enthesis.
- Avoid intratendinous spread into adjacent gluteal or paraspinal tendons unless intentionally treating them.
- Combine with a load-management plan (hip hinge mechanics, posterior chain strength, lumbopelvic stabilization) to reduce recurrence.
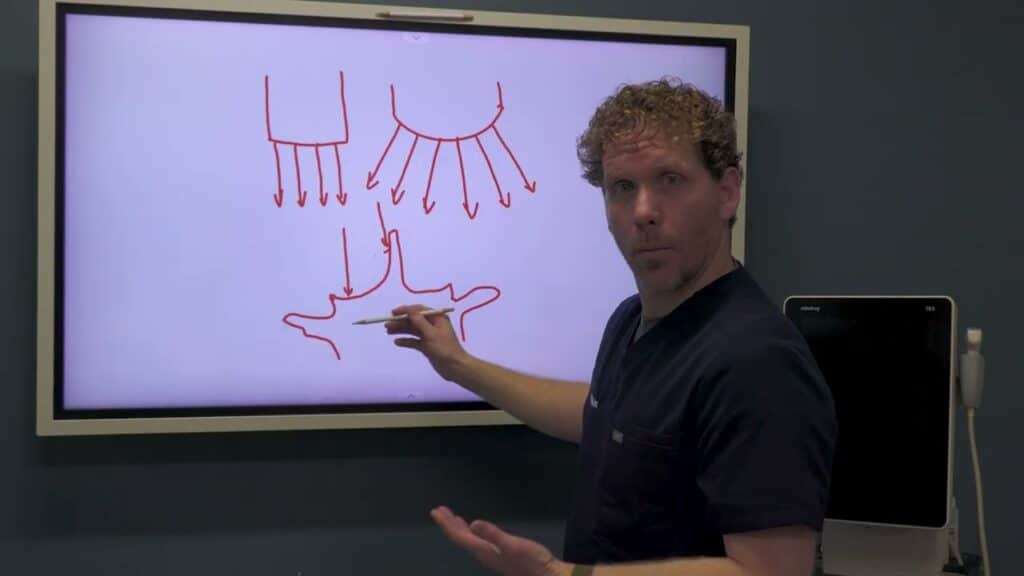
Why this matters
The PSIS-level TLF is a high-yield pain generator in axial LBP and often overlooked when imaging focuses only on discs or facet joints. Systematic ultrasound evaluation of deep vs superficial bands lets you localize pathology and treat precisely, often producing meaningful relief in patients who’ve “tried everything.”