The 5-Minute Consult: Patient Education That Drives Outcomes
Great procedures start with great conversations. When knee pain patients arrive already “pre-sold” by a friend’s success, your job is to connect clear diagnostics with an ethical, evidence-based plan they understand—and can act on. Here’s a fast, reproducible flow you can use at the end of your visit to align expectations, reduce fear, and map next steps.
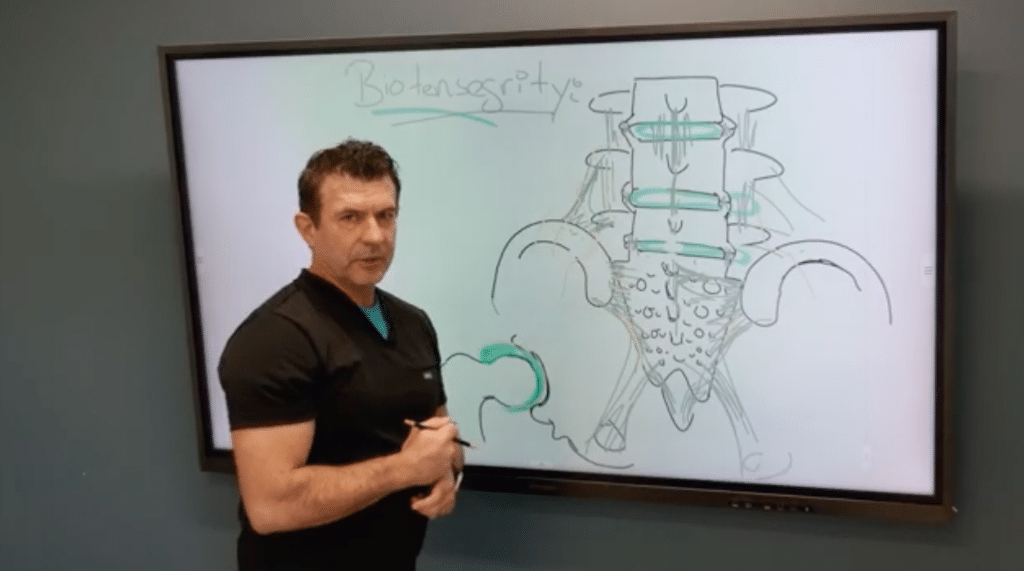
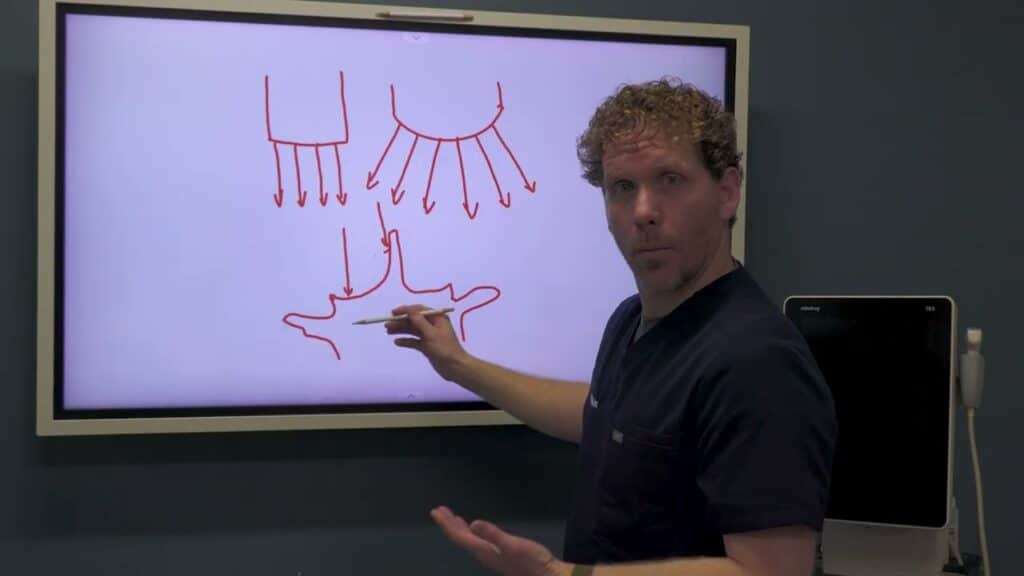
1) Make the invisible visible
Use a whiteboard, tablet, or smart board. Sketch the hinge joint, label medial and lateral compartments, and mark the patient’s pain zone. Briefly show how cartilage loss, a partially resected/extruded medial meniscus, patellar maltracking, and MCL laxity create abnormal loading. Patients remember pictures.
2) Synthesize the findings
Tie history, exam, ultrasound, and X-ray into three or four clear diagnoses:
- Knee osteoarthritis (cartilage thinning + risk factors)
- Medial meniscal pathology (tears/extrusion; not currently locking → likely nonsurgical)
- Patellofemoral maltracking (lateral tracking, anterior knee pain)
- Neuropathic contributors (periarticular genicular/saphenous branches can amplify pain)
Explain that nerves modulate pain and healing; if you ignore them, you may undertreat.
3) Set treatment goals (pain now vs healing later)
Patients want to move, travel, and sleep. State two parallel aims:
- Reduce pain now to enable activity and PT
- Improve tissue environment for longer-term function
4) Present the ladder of options
Avoid rushing to surgery or high-dose steroids (discuss risks and cartilage effects).
A. Low-risk relief
- Dextrose (D5W) perineural “nerve reset” around symptomatic branches
- Intra-articular dextrose for joint pain modulation
B. Insurance-covered adjuncts
- Viscosupplementation (“lube job”) when criteria met (often requires ~4 PT sessions)
- Targeted PT for tracking and strength (VMO, hip abductors/ERs)
- Unloader brace to open the medial compartment during activity and during post-procedure protection
C. Regenerative options (orthobiologics)
- PRP (platelet concentrate as the “fertilizer” for healing signals)
- Bone marrow–derived cell therapy (the “seed”); often combined with PRP for synergy
Set expectations, discuss indications/contraindications, and review evidence you provide in take-home materials.
5) Optimize the terrain
Address modifiable risks that blunt outcomes:
- Hormonal status (e.g., menopause): consider functional medicine consult and labs
- Supplements with supportive evidence (e.g., omega-3, turmeric, vitamin D/C) and dosing sheet
- Load management (brace use, graded activity)
6) Close with a clear plan + follow-through
Number your handouts (1–4), summarize in one minute, and schedule:
- Today: nerve/joint pain modulation; brace fitting; PT referral
- Next 1–2 weeks: insurance steps, functional medicine consult, supplements
- 5–6 weeks: reassess; consider PRP/BMAC based on response and goals
Reinforce via automated email/SMS (testimonials, steroid education, procedure FAQs). Use an AI scribe to capture your narrative as you teach—the same words educate the patient and build a clean chart.
Bottom line
Show the problem, name the drivers (joint + nerve + mechanics), and offer a stepped plan that relieves pain now while creating the conditions for healing. Patients feel heard, you set realistic expectations, and your procedures work better.