How to Approach the Lumbar Spine: A Practical Guide for Diagnosing and Treating Low Back Pain (Part 1)
How to Approach the Lumbar Spine: A Practical Guide for Diagnosing and Treating Low Back Pain (Part 1)
When a patient arrives with low back pain, the goal is clear: identify the pain generators and assemble a treatment plan that reduces pain, improves function, and preserves the health of the structures involved. In this guide, I’ll walk through a practical framework you can apply in clinic, with a focus on anatomy, diagnostics, and a stepwise approach to treatment that includes conservative care, injections, and regenerative techniques.
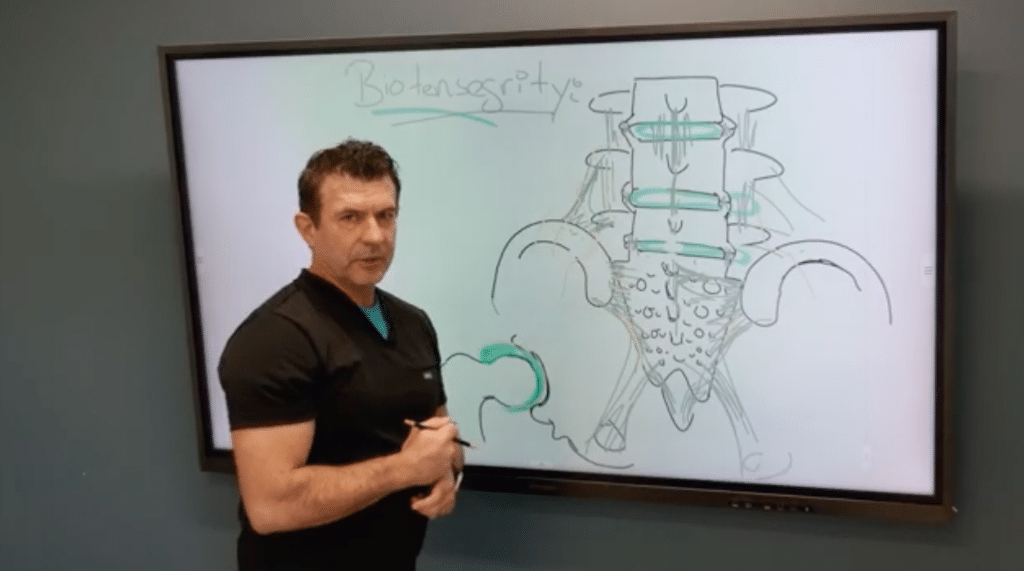
First, anchor your assessment in a solid understanding of the lumbar–sacral complex. The spine is a stack of bones with joints between them, stabilized by a network of ligaments and a surrounding joint capsule. Visually, imagine bone–disc–bone–disc along the lumbar spine, with the sacrum and ilia completing the pelvic connection. The ligaments act like a structural “duct tape,” holding the joints together and guiding movement. This integrative view matters because pain rarely comes from a single structure; it often reflects the interplay of bones, discs, ligaments, and the joints they form.
A critical hotspot to assess is the L5–S1 transition. This junction bears a lot of biomechanical and loading stress, and it’s a common source of wear, instability, and pain. L5–S1 stability depends on a robust set of ligaments, and in this region you’ll often find that the ligamentous anatomy is thinner or less robust, making the area particularly vulnerable to degeneration and inflammatory changes. When evaluating this segment, pay attention to the disk space as well as the surrounding ligamentous attachments. MRI and radiographs can reveal degenerative changes, but the clinical picture—where the patient feels pain, what movements provoke it, and what reproduces symptoms—will guide your next steps.
Beyond the L5–S1 junction, the sacral–iliac region (the SI joints) and the posterior pelvic ligaments deserve careful attention. The sacrum hosts a network of short and long ligaments that connect the ilium to the sacrum and provide both stability and subtle mobility. When you’re parsing pain in this area, consider the short sacroiliac ligaments that attach along the ilium and sacral crests, as well as the deep interosseous ligaments that act as some of the strongest stabilizers in the pelvic ring. These ligaments can be underdiagnosed as contributors to axial low back pain, yet ultrasound and targeted injections can reveal their involvement and offer therapeutic options.
Ultrasound and dynamic testing become powerful tools once you’ve identified the ligamentous landscape. With appropriate imaging, you can visualize attachment sites and guide injections to stabilize specific ligaments or ligament complexes. A practical approach is to map the bony landmarks (such as the sacral crests, spinous processes, and tubercles) and then correlate these with palpable and ultrasound-visible ligament orientations. The goal is to restore stability to the posterior elements so that the joints move with controlled, less painful mechanics.
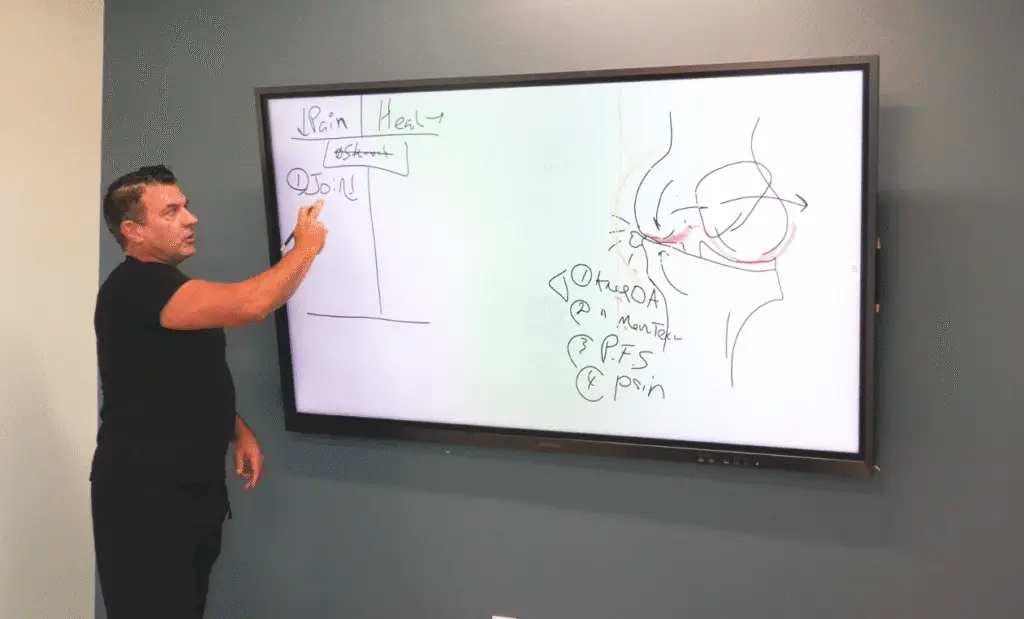
Treatment, in practice, is multimodal. Start with conservative measures—physical therapy to improve strength and flexibility, activity modification, and bracing when indicated. If conservative measures don’t yield sufficient relief, consider targeted interventions such as nerve blocks or epidurals to break the pain cycle and enable rehabilitation. Finally, for patients with focal ligamentous instability or degenerative changes where traditional therapies fall short, regenerative procedures that target joints, ligaments, fascia, and muscle–tascue interfaces can offer meaningful improvements in pain and function. The unifying theme is to tailor strategies to the patient’s unique anatomic and biomechanical profile, not to rely on a one-size-fits-all protocol.
As you expand your practice, you’ll develop a more nuanced sense of which structures to test and treat first. The more proficient you become at recognizing the ligamentous architecture and its role in stability, the more precise your injections, blocks, and rehabilitative plans will be. With careful assessment and a thoughtfully staged treatment plan, you can help patients achieve durable reductions in pain and meaningful gains in function.