Pelvic Nerves and Ligaments in Lower Back Pain: Understanding Entrapment and Relief Strategies (Part 2)
Pelvic Nerves and Ligaments in Lower Back Pain: Understanding Entrapment and Relief Strategies (Part 2)
Lower back pain is a common and complex symptom with many potential drivers. Among these, the pelvic-lumbar region harbors a network of ligaments and nerves that can influence pain patterns even when the discs or joints appear non-acute. Understanding how these structures interact helps clinicians and informed patients approach assessment and relief in a more targeted and safe way. This post offers a practical framework for recognizing how pelvic ligaments and nerves may contribute to pain, what non-invasive assessments can reveal, and how to discuss safe, evidence-based strategies with a clinician.
Anatomy and Stability
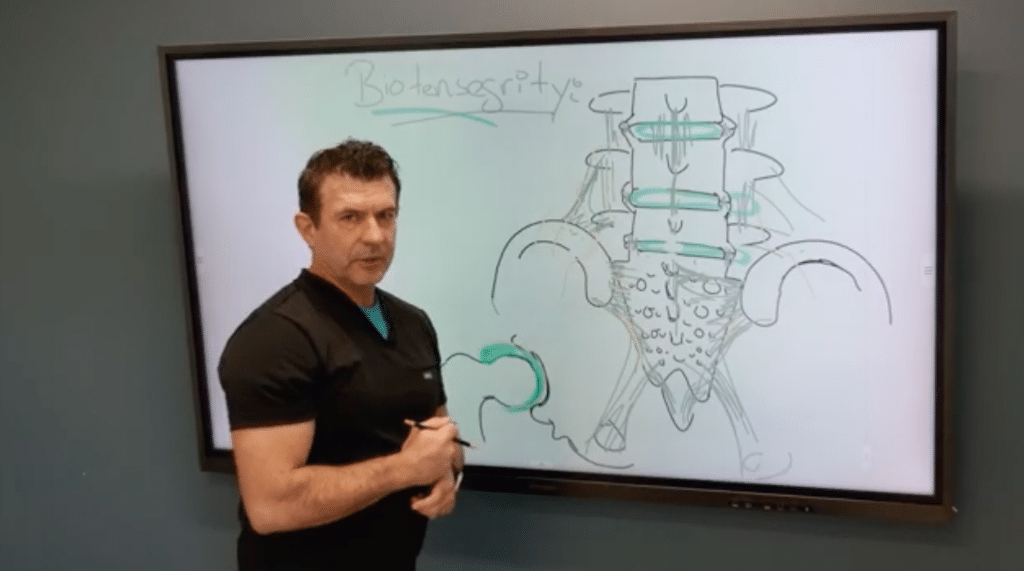
Ligaments and Pelvic Support The spine is stabilized by a lattice of ligaments and connective tissues that connect the spine to the pelvis. In the lower back, several ligaments play key roles in maintaining alignment and supporting movement. The interspinous and intertransverse ligaments, along with the iliolumbar ligaments, help stabilize the lumbar region and connect to the sacrum and iliac bones. A family of pelvic ligaments known as the C ligaments adds to this complex network. Short and long fibers blend with surrounding tissues, contributing to overall pelvic stability. When instability or tightness arises, these structures can influence pelvic mechanics and potentially affect nearby nerve pathways. This is not to suggest every pain arises from these ligaments, but recognizing their role can broaden your diagnostic and therapeutic options.
Nerve Entrapment
How Pain Can Emerge A useful way to think about back and pelvic pain is to consider nerves that traverse the pelvis and lumbar region. As nerves exit the spine and pass near ligaments and bony landmarks, they can become irritated if tissues shift or stiffen. A representative pathway involves a nerve that travels near the iliac crest and crosses pelvic ligaments as it courses toward the buttock and thigh. When surrounding tissues or joints rotate or become stiff, these nerves may experience tension or compression, leading to pain that radiates or feels burning, sometimes with numbness or tingling. Clinically, researchers and clinicians look for pain reproduction with palpation over the iliac crest and particular ligament regions, and they consider whether targeted interventions might relieve nerve irritation while protecting overall safety and function.
Assessment and Safe Considerations
A practical assessment approach emphasizes non-invasive, collaborative exploration with a clinician. Start with careful palpation around the iliac crest and sacroiliac region to identify focal tenderness. Observe movement for signs of abnormal pelvic rotation or instability, as these patterns may correlate with nerve irritation. A neurologic screening helps distinguish nerve-related signs from other sources of pain. It’s important to emphasize that this overview is educational and not a substitute for professional diagnosis. If you’re experiencing persistent back or pelvic pain, seek a qualified clinician who can perform a comprehensive evaluation, including physical examination and, when appropriate, imaging or diagnostic tests.
Treatment Concepts and Cautions
In the context of pelvic instability and nerve irritation, treatment goals focus on safety, symptom relief, and restoring healthy function. A clinician might discuss strategies to reduce nerve irritability and local inflammation while avoiding procedures that are not indicated. Any approach should be tailored to the individual’s health status, activity goals, and risk factors, with careful consideration of consent, safety, and evidence-based practice. Educational conversations with patients should cover what to expect, potential risks, and the rationale for each recommended step. The aim is to support informed decision-making and a shared plan of care rather than a single “cure.”
Takeaways for Patients and Clinicians
The pelvic ligaments and nerves contribute to a complex picture of lower back and pelvic pain. Nerve irritation can arise from mechanical instability, joint changes, or ligament tightness, and a careful, evidence-based assessment guides safe, individualized treatment. Collaboration among clinicians, therapists, and patients improves outcomes by combining education with targeted strategies. Even when a single structure seems implicated, a broader view that integrates the whole pelvic-lumbar system often yields the most reliable path to relief.
Next Steps
For clinicians, consider a structured assessment that integrates pelvic mechanics, neural pathways, and patient-reported symptoms, potentially coordinating with physical therapy and medical evaluation. For patients, discuss pelvic stability and nerve pathways with your clinician to learn about diagnostic steps and personalized treatment options. If you’re seeking further guidance, request a consultation to discuss a tailored evaluation plan that aligns with your goals and safety.