Sharpening Ultrasound Skills for Spinal Injections: A Practical How-To for Providers
Sharpening Ultrasound Skills for Spinal Injections: A Practical How-To for Providers
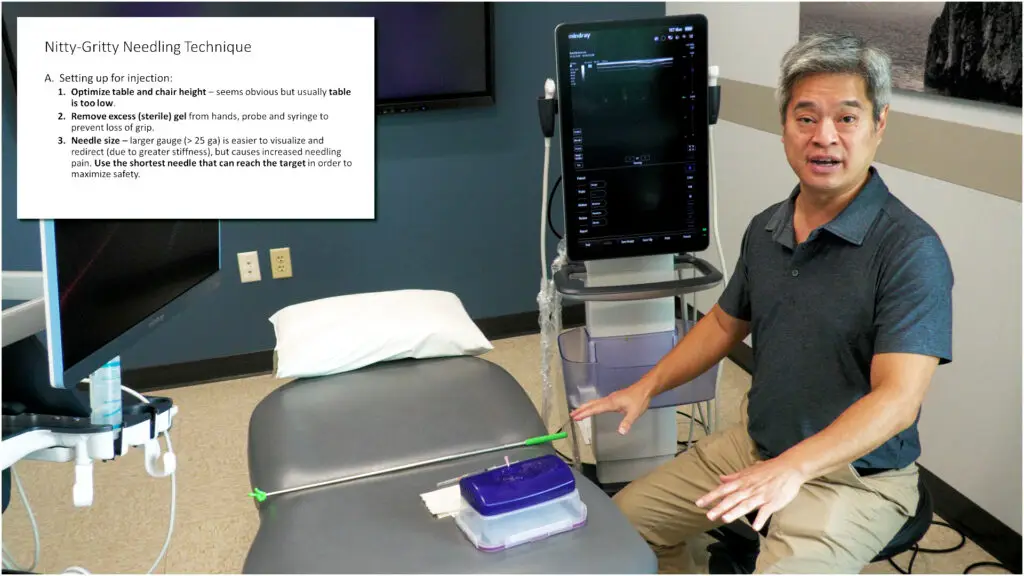
Before you start scanning, clarify your goals. Identify the target anatomy for your planned injection—whether you’re aiming for the spinous process, lamina, facet joints, or transverse processes. Mapping out your needle trajectory and entry angles ahead of time helps you select the most appropriate transducer and scanning window. Establishing these parameters upfront sets the stage for a smoother, more precise procedure.
Transducer selection is central to this process. The curvilinear transducer, typically lower in frequency with a larger footprint, excels when target depth is a factor. For structures around five centimeters or deeper, it provides better penetration and a broader field of view, enabling you to visualize deep bony landmarks and the needle path with greater confidence. A key advantage of the curvilinear probe is its multi-angle sound-wave emission, which can improve visualization when you plan multiple needle angles during the injection.
By contrast, the linear transducer offers higher near-field resolution and is superb for superficial structures—roughly zero to four centimeters deep. It provides detailed visualization of the superficial bone cortex and soft tissue, which can be crucial for precise needle localization once the trajectory is established and the target lies within the near field. A practical approach is to start with curvilinear for depth and broad overview, then switch to linear for final needle advancement and fine-tuning in the near field.
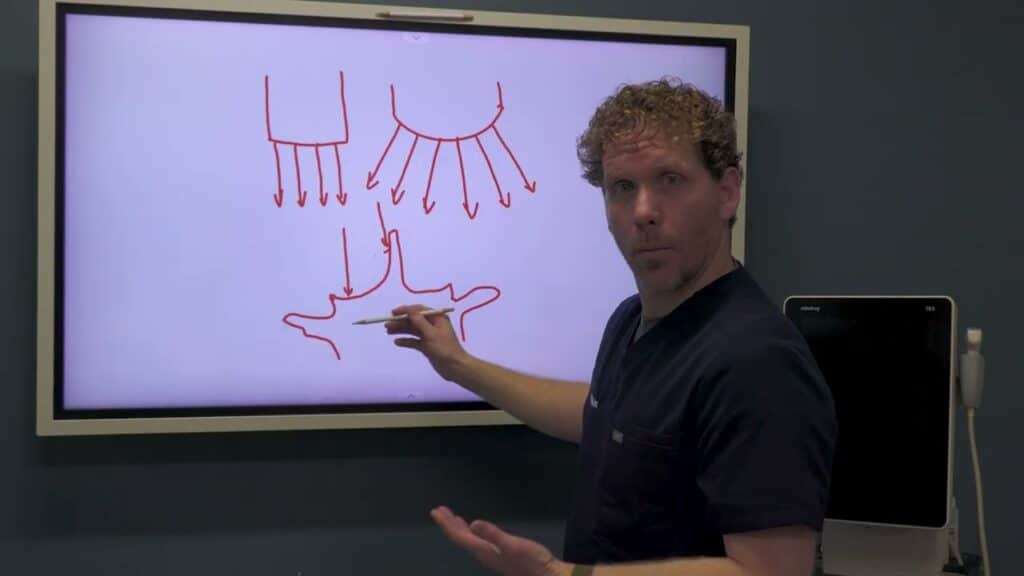
Imaging the spinal cortex and landmarks benefits from understanding how the angle of insonation affects reflection. Perpendicular insonation yields the brightest reflections from cortical bone, so position the transducer to maximize perpendicular impact on the spinous processes, lamina, and facet joints. With a curvilinear probe, you can take advantage of multiple incident angles to enhance visualization of complex anatomy and to track the needle when approaching from multiple directions. If you encounter artifact or shadowing, a small adjustment in angle or a gentle rock of the probe can optimize reflections from the cortical bone.
Transducer selection is more than a procedural backdrop; it’s a lever that can meaningfully improve accuracy, safety, and efficiency. By understanding the trade-offs between curvilinear and linear probes and applying deliberate imaging strategies, clinicians can elevate their ultrasound-guided spinal injections and deliver better patient care.
Sharpening Ultrasound Skills for Spinal Injections: A Practical How-To for Providers Read Post »