Deliberate Offset in Palpation-Guided Prolotherapy: Safe, Gradual Needle Progression (Part 1)
Deliberate Offset in Palpation-Guided Prolotherapy: Safe, Gradual Needle Progression (Part 1)
I’m Dr. David Wang from RPI, sharing a practical, clinician-focused approach to improving safety and accuracy in palpation-guided, non-image-guided prolotherapy injections. This is Part 1 of a two-part series designed to give you a robust framework you can apply in daily practice when navigating the shoulder’s upper joint without real-time imaging.
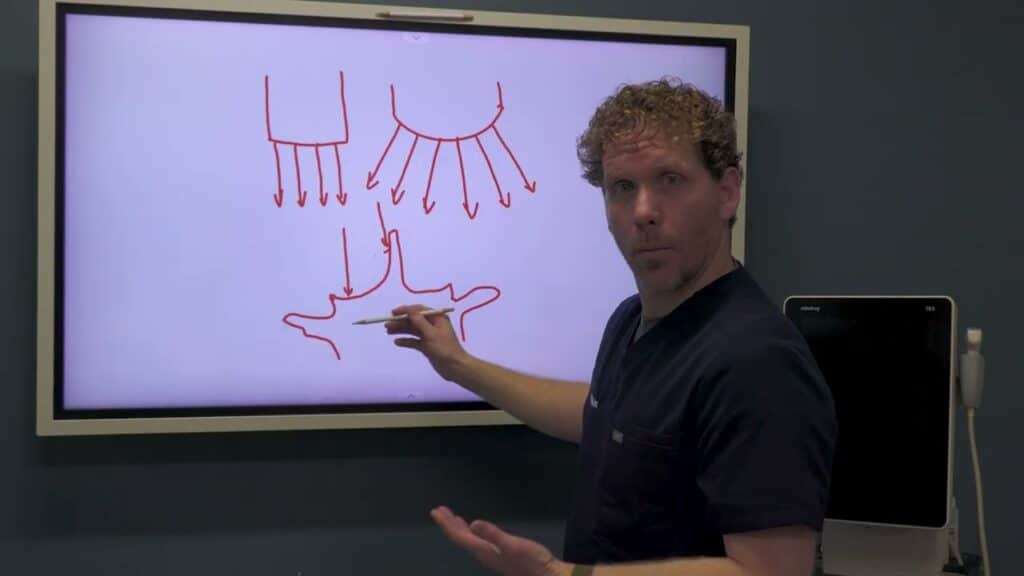
The central idea I want to convey is deliberate offset. This concept, borrowed from military training, helps you establish a reliable reference point when you don’t have an imaging modality guiding you. In injections around the shoulder, you often face a challenge: you’re unsure exactly where you are in relation to deep osseous landmarks and adjacent neurovascular structures. Deliberate offset asks you to take a controlled misdirection initially—move superficially or off-target by a small margin—so you can confirm your relative position against a known landmark before steering toward your actual target.
To illustrate, imagine your objective is the upper portion of the joint, with nearby neural structures as a cautionary reminder. You begin by entering at a very shallow angle, nearly parallel to the skin, deliberately avoiding bone on the first pass. This initial superficial pass tells you you’re safely above the surface and gives you a baseline for tissue depth. From there, you progressively increase the angle in small increments—five degrees at a time—while monitoring how much needle is exposed. A key cue is the needle’s depth: you’ll often notice the exposure decrease as you begin to approach the target plane, then suddenly plunge deeper once you cross a shallow-to-deep transition. That moment—the gummy sensation of the needle contacting deep tissue or bone—signals you’ve reached the correct osseous region for the prolotherapy injection.
This method has two powerful benefits. First, it provides a safer, more controlled path to a deep target, reducing the risk of accidentally traversing into neural foramina or misplacing the needle. Second, it offers a repeatable workflow across patients with different body habitus. By starting superficially and gradually offsetting deeper, you create a reliable, patient-specific trajectory that you can adjust in real time.
In the context of shoulder injections, the deliberate offset technique helps you localize the upper joint region with improved confidence. It’s particularly useful when landmarks are ambiguous or when you’re working near complex structures where precision matters for safety and efficacy. The technique is not a substitute for imaging guidance when it’s available, but it’s a valuable skill set for clinicians performing palpation-guided injections in regenerative medicine.